GALLBLADDER
Gallstones
On this page you can find:
* What are gallstones?
* What causes gallstones?
* Who is at risk for gallstones?
* What are the symptoms of gallstones?
* How are gallstones diagnosed?
* How are gallstones treated?
* Do people need a gallbladder?
* Key points
What are gallstones?
Gallstones are small, pebble-like substances that form in the gallbladder. The gallbladder is a small pear-shaped sac located under the liver in the upper right abdomen. Stone-like gallstones are formed as a result of the hardening of the concentrated bile fluid residue stored in the sac in pieces. Bile especially helps digest fats. Bile is made in the liver and stored in the gallbladder. Then, with the contraction of the gallbladder during the meal, the bile passes into the small intestine via the bile ducts to aid digestion.
Bile contains water, cholesterol, fat, bile salts, protein and bilirubin, a waste product. Bile salts break down fats, making them easier to digest. Bilirubin gives bile and stool a yellowish-brown color. If the bile contains a high amount of cholesterol, and a small amount of bile salts in bilirubin, it causes the formation of gallstones.
There are two types of gallstones: cholesterol and pigment stones. Cholesterol stones are usually yellow-green in color and primarily contain hardened cholesterol. Cholesterol stones make up about 80 percent of gallstones. Pigment stones are small, dark stones made from bilirubin. Gallstones can be as small as a grain of sand or as large as a golf ball. Gallstones can develop as a single large stone or hundreds of small stones, or a combination of the two.
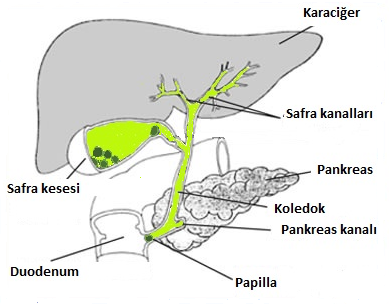
Schematic view of the gallbladder, liver, pancreas, duodenum and biliary tract (stone appearance in the gallbladder and papilla).
Gallstones that pass from the gallbladder into the bile ducts (choledochus) can block the normal flow of bile from the liver to the small intestine. The bile ducts are as follows.
* Hepatic ducts carry bile out of the liver.
* The cystic duct is between the gallbladder and the main duct.
* Choledochus (main duct) transfers bile from the hepatic duct and cystic duct to the small intestine.
As a result of obstruction of bile flow in the main bile duct, infection may develop in the gallbladder and biliary tract. In addition, bile trapped in these ducts can, in rare cases, cause inflammation in the liver. Another duct that opens into the common bile duct is the pancreatic duct, which carries the digestive enzymes of the pancreas out of the pancreas. Gallstones that pass into the main bile duct can sometimes block the flow in the pancreatic duct, causing an extremely serious and dangerous condition called pancreatitis.
If the obstruction of the main bile ducts (choledochus) continues for a long time, severe infection or damage to the gallbladder, liver and pancreas can occur. The main signs of this serious problem are fever, jaundice, and persistent or intermittent severe pain. It is a condition that needs to be treated urgently. If left untreated, the condition can be fatal.
What causes gallstones?
Scientists believe that cholesterol stones form when bile contains too much cholesterol and bilirubin contains small amounts of bile salts. The exact cause of this imbalance is not known. In addition, incomplete or insufficient emptying of the gallbladder is an important factor in the formation of gallstones.
The cause of pigment stones is not known exactly. Pigment stones tends to occur more often in people who have liver cirrhosis, or disorders that cause the liver to generate too much bilirubin, as well as inherited blood diseases such as sickle cell anemia.
The presence of gallstones can cause more gallstones to form in the bladder. Other factors that cause gallstones, especially cholesterol stones, are listed below.
* Gender. Gallstones develop in women twice as often as in men. In cases where estrogen levels increase, such as pregnancy, hormone replacement therapy and use of birth control pills, bile cholesterol levels increase and the contraction of the gallbladder is not complete. In both cases, they are the most important factors in the formation of gallstones. Estrogen and progesterone (female hormones) cause relaxation in smooth muscles. They are smooth muscles that contract the gallbladder wall. Therefore, in women, especially in cases where the hormone level is high, the gallbladder cannot be emptied sufficiently. In the non-emptying bladder, it is easier to petrify the bile debris.
* Family history. Gallstones are more common in those with a family history of gallstones.
* Weight. In many clinical studies, even being moderately overweight has been shown to increase the risk of gallstone formation. The reason is probably the increase in the cholesterol level in the bile and the decrease in the bile salts level. Increased cholesterol reduces gallbladder emptying. Obesity is an important risk factor for gallstones, especially in women.
* Diet. High fat and cholesterol, low fiber diet causes high cholesterol in bile. This increases the risk of gallstone formation due to decreased gallbladder emptying and increased bile cholesterol level.
* Fast weight loss. The body metabolizes fat during prolonged fasting and very strict diets that cause rapid weight loss. As a result, additional cholesterol is secreted in the liver and can cause gallstone formation.
* Age. People over the age of 60 are more likely to develop gallstones than younger people. As people age, the body tends to excrete more cholesterol into the bile.
* Cholesterol lowering drugs. Drugs that lower blood cholesterol levels actually increase the amount of cholesterol secreted in the bile. In turn, the risk of gallstones increases.
* Diabetes. People with diabetes often have high levels of fatty acids called triglycerides. These fatty acids can increase the risk of gallstones.
Who is at risk for gallstones?
Those at risk for gallstones include:
* women - especially those who are pregnant, using hormone replacement therapy or birth control pills
* women who have given birth numerous times
* People over 60 years old
* overweight or obese men and women
* people who lose weight very fast
* people with a family history of gallstones
* people with diabetes
* people taking cholesterol-lowering medication
What are the symptoms of gallstones?
When gallstones move into the bile ducts, congestion occurs, the pressure in the gallbladder increases and many different symptoms can develop. Symptoms due to bile duct obstruction appear suddenly and are called gallbladder attack (cholecystitis). A gallbladder attack can occur overnight, usually following fatty meals. A typical attack can cause:
* Right upper abdominal pain lasting from 30 minutes to several hours
* back pain between the shoulder blades
* pain under right shoulder
If you think you are having a gallbladder attack, let your doctor know. Although these attacks due to gallstone movement usually pass, infection and perforation of the gallbladder may develop.
People with any of the following symptoms should contact a doctor immediately:
* Prolonged pain - more than 5 hours
* nausea and vomiting
* fever and chills
* yellowing of eyes and skin
* clay-colored (white) stool
Many patients with gallstones may have no symptoms. These stones are called "silent stones". These stones do not impair gallbladder, liver and pancreatic functions and do not require treatment.
How are gallstones diagnosed?
Gallstones are usually discovered during tests for other diseases. When gallstones are suspected, the first diagnostic method is ultrasonography. The order followed in diagnostic methods is as follows
* Ultrasonography. It is the first diagnostic method used when gallstones are suspected as a result of the patient's complaints and examination findings. It is the most sensitive and reliable method in the diagnosis of gallstones. A hand-held probe is placed on the patient. Sound waves are sent to the liver and gallbladder through this probe. The echoes of the sent sound waves create an electrical impulse, which is viewed as a picture on a monitor. If you have gallstones, sound waves create the loudest echo.
* Computed tomography (CT). CT scanning is a non-invasive method. Cross-sectional images of the body are obtained with X-ray. It is a diagnostic method used in the diagnosis of gallstones or complications of gallstones such as infection and perforation.
* Magnetic resonance (MR). MR cholangio-pancreatography is a non-invasive method. It is a valuable diagnostic method in the diagnosis of stones that have passed to the main bile ducts (choledochal stones) rather than in the diagnosis of gallstones.
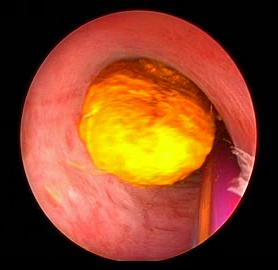
* Endoscopic retrograde cholangiopancreatography (ERCP). ERCP is an invasive method used to diagnose and remove stones in the bile ducts. The endoscope, which has a light and a camera on its tip, is advanced under sedation through the mouth and stomach to the duodenum. The other end of this endoscope is integrated into a video-monitor. First, an opaque substance is administered to the bile ducts through the papilla to determine whether there is a stone or not. If there are stones, the papilla is enlarged and the stones are lowered into the duodenum with a basket or balloon.
* Blood tests. Blood tests give important information on the course of the disease and its complications when there are signs of infection, pancreatitis obstruction or jaundice.
Since gallstone symptoms can be similar to those of heart attack, appendicitis, ulcer, irritable bowel syndrome, hiatal hernia, pancreatitis and hepatitis, they can be confused with these diseases. Therefore, correct diagnosis is very important.
How are gallstones treated?
Surgery
Sometimes no treatment is needed if you have gallstones without symptoms. This rule applies to patients over 50 years of age who are diabetic and have a small number of stones without hemolytic blood disease. If you suffer from gallstones and have frequent gallbladder attacks, your doctor will suggest you have the gallbladder removed. This surgery is called "cholecystectomy". The gallbladder is an organ that is not essential for life. Cholecystectomy is one of the most commonly performed surgeries today.
Almost all cholecystectomies are performed by the laparoscopic method. Laparoscopic cholecystectomy is performed under general anesthesia with 3 or 4 incisions 0.5-1 cm wide. Recently, it is also done with a single incision 2-3 cm wide. A telescope with a video-camera at its tip is inserted into the abdomen. The intra-abdominal image is magnified by the video-camera and transferred to the monitor. The surgeon observes the intra-abdominal image on the monitor and performs the operation with instruments placed in the abdomen at the other two insertion sites.
Recovery after laparoscopic surgery is faster than the open method. Laparoscopic method has many advantages compared to open surgery.
* short hospital stay (one night)
* time to return to normal activity is short (4-5 days)
* less pain after surgery
* Complications such as wound infection and surgical site hernia are almost non-existent
* cosmetic results are excellent.
Open surgery is preferred for gallbladder removal when advanced infection, abscess, and perforation are detected in the gallbladder as a result of the examinations. In some cases, open surgery is planned and performed. However, sometimes these problems are seen or occur during laparoscopy and open surgery is mandatory. The rate of conversion to open surgery during laparoscopy is between 2-5%. The hospital stay after open surgery is 3-5 days, and the time to return to normal activities is about one month. Since there is a 10-12 cm muscle incision in the anterior abdominal wall, postoperative pain is more.
The most common complication of gallbladder surgery is bile duct injury. As a result of bile duct injury, bile may pass into the abdominal cavity and cause a serious infection. Mild injuries can sometimes be treated with non-surgical methods. However, major injuries are more serious and require additional surgical intervention.
Gallstones can sometimes coexist in the bile ducts with the gallbladder. In this case, with ERCP, cholecystectomy can be performed after removing stones in the duct first. However, nowadays, instead of this two-stage procedure, "one-stage procedure", that is, performing ERCP and cholecystectomy in the same session is gaining popularity. In addition, during laparoscopic cholecystectomy, choledochal stones can be surgically removed by opening the bile ducts (See. Video-Laparoscopic choledoch exp.). Sometimes, gallstones in the bile ducts can be diagnosed in the patient weeks, months, or even years after cholecystectomy surgery. In such cases, ERCP is performed and stone removal is usually successful.
Non-surgical treatment
Non-surgical approaches are applied for cholesterol stones in patients whose general condition is severely poor and who are at high risk for surgery.
Stones treated with non-surgical methods usually recur within 5 years.
* Oral dissolution therapy. Medicines made from bile acid are used to dissolve gallstones. These drugs are known as ursodeoxycholic acid (Ursofalk) and chenodeoxycholic acid (Chenofalk) and are very successful in dissolving small cholesterol stones. It may take months or years for all stones to dissolve. Both drugs can cause mild diarrhea, and chenodeoxycholic acid can temporarily raise blood cholesterol and liver enzyme levels.
* Contact dissolution therapy. In this experimental procedure, a drug is injected directly into the gallbladder to dissolve cholesterol stones. The drug named methyl tert-butyl ether can dissolve the stones in 1-3 days, but it causes irritation and some complications have been reported. The procedure is being tested in symptomatic patients with small stones. This method has not yet entered into routine practice.
Do people need a gallbladder?
Fortunately, the gallbladder is not an essential organ for humans. The gallbladder is an organ that we can live without. The liver produces bile to digest a normal meal. It is stored in the gallbladder and emptied into the small intestine with food. After the gallbladder is removed, the intrahepatic bile ducts and the common bile duct expand and store bile. The stored bile flows into the common bile duct instead of the gallbladder through hepatitic ducts and then directly into the small intestine. Residual bile flows into the small intestine at more frequent intervals. As a result, soft and more frequent stools may occur in approximately 1 percent of patients. Some patients may also have indigestion and gas problems. But these changes are usually temporary, if they persist you should contact your doctor.
Key points
* Gallstones form when a precipitate of condensed bile hardens in the gallbladder.
* Gallstones are more common in older adults, women, people with diabetes, those with a family history of gallstones, people who are overweight (obese) or lose weight rapidly, and those taking cholesterol-lowering medication.
* Gallbladder attack often occurs after eating, especially after a fatty meal.
* Symptoms can mimic many other diseases, including a heart attack. Therefore, correct diagnosis is important.
* If you have complaints about gallstones, it is beneficial to have surgery before complications such as inflammation, abscess, perforation and jaundice develop.
* Gallstones can cause serious problems if they pass into the bile ducts and become blocked.
* Laparoscopic removal of the gallbladder is the most preferred treatment method.
Assoc. Prof. Ahmet Tekin

General Surgeon