MINI GASTRIC BYPASS
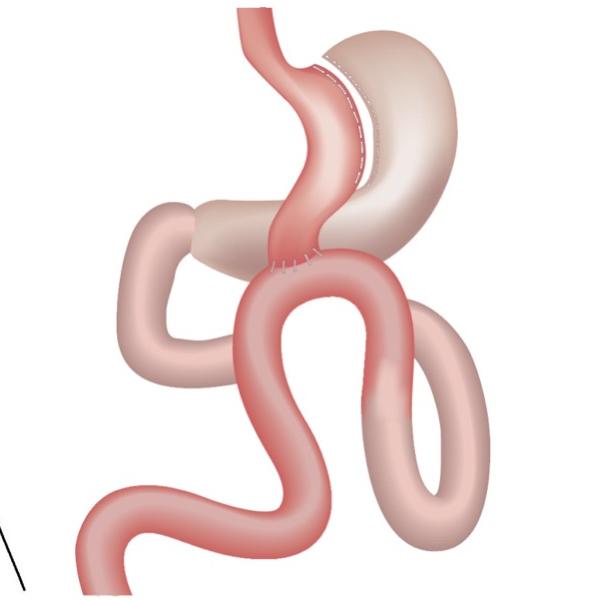
It is a method that has emerged as an alternative to Roux en Y Gastric Bypass surgery and has been popular in recent years. Compared to gastric bypass, it is technically simpler and the surgery duration is shorter. Complications are less than traditional gastric bypass. It is an operation that restricts food intake and impairs food absorption. In this technique, a gastric tube is first created, similar to sleeve gastrectomy surgery, but smaller in size. Then, the first 150-200 cm of the small intestine is disabled and the small intestine is ligated to the lower end of the newly formed tube stomach.
After mini gastric bypass, weight loss occurs in patients with 3 different mechanisms.
Food intake is restricted by gastric sleeve.
Food absorption is reduced by deactivation of the first 150-200 cm of the small intestine.
The level of hormonal changes (hunger hormone-ghrelin) decreases.
The surgery is performed laparoscopically (closed) as in other procedures. The operation is made from 4-5 holes smaller than 1 cm opened on the abdomen. The postoperative period is the same as in the classical gastric bypass.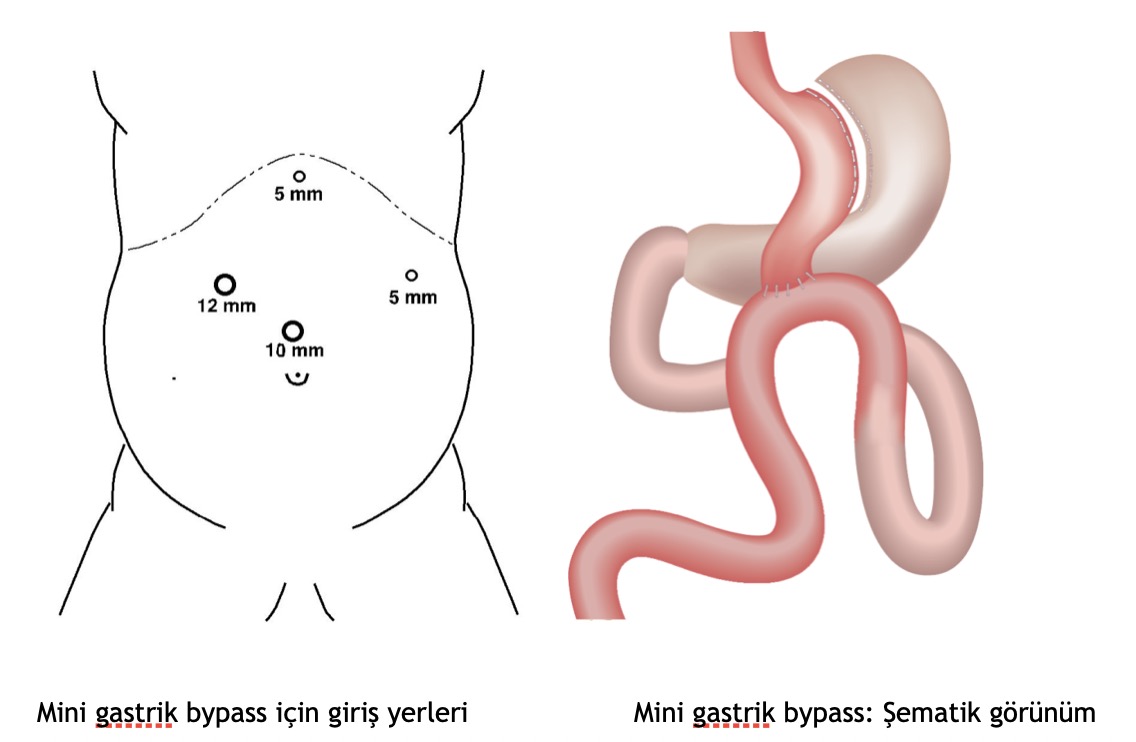
To Whom MGB Should be Applied?
Mini gastric bypass method is preferred in the treatment of insulin-dependent morbidly obese patients. It is more effective in diabetic patients compared to sleeve gastrectomy and classical gastric bypass surgery. In addition, mini gastric bypass is recommended in patients who are extremely obese (BMI>50 – “super obeseâ€) or in patients with obvious type 2 diabetes.
Mini gastric bypass is usually the preferred method for patients who have had sleeve gastrectomy/stomach reduction surgery and gained weight again after years and become morbidly obese. In these patients, mini gastric bypass is easy and has few complications. The 1st stage of the operation (tube stomach) has already been performed. The second phase will be added.
After surgery!
Postoperative hospital stay is 3-4 days. Patients are usually kept in intensive care units for the first 1 or 2 days.
The patient is mobilized 1 day after the operation.
A catheter (tube) can be placed in the stomach for 2-3 days.
During the first 2 days it will not be possible to eat. If there is no risk of leakage, watery food is begun to be consumed after the 3rd day and then continues with mashed or soft foods.
A tube can be placed from the nose to the stomach for 2-3 days to empty the stomach contents after the surgery.
Special socks are worn on the feet and legs to help prevent the formation of blood clots.
Medicine (heparin) is administered to prevent blood clots from forming.
Painkillers are given intravenously for pain
Possible complications are similar to Roux en Y Gastric bypass surgery. Vitamin (B1, B6, B12, Folic acid, D) and electrolyte (Fe, Ca) deficiencies that occur due to absorption deficiency are similar to Roux en Y Gastric Bypass but occur more frequently. In the postoperative period, multivitamins (supradyn, pharmaton, etc.) are administered to prevent vitamin and mineral deficiencies. In addition, patients are checked every three months and their vitamin and mineral values are measured. Additional supplements are prescribed when a deficiency is observed.
What are the benefits of gastric bypass?
Most people lose 10 to 15 kg in the first month after surgery. The rate of weight loss will decrease over time. The success rate of losing excess weight after mini gastric bypass is higher than sleeve gastrectomy. In both methods, food intake is limited. However, food absorption is additionally decreased in gastric bypass. Therefore, it is relatively superior to tube stomach in losing excess weight. It is also superior to sleeve gastrectomy surgery in the treatment of Type 2 diabetes.
Within 1 year after the operation, 75% of excess weight is lost. Loss of excess weight reaches 80-90% in the second year. With the loss of excess weight, a significant improvement is also observed in diseases that accompany obesity. A person can regain self-confidence. In addition, with the significant decrease in the load on the knee and waist, most of the knee and low back pain will go away on its own.
OBESITY-RELATED DISEASE
RECOVERY RATE (%)
Asthma
82
Hypertension
60-70
High cholesterol level
94
Obstructive sleep apnea
75
Osteoarthritis of the knee and foot joints
85
Type 2 diabetes
80-85
Depression
72
Mini gastric bypass compared to Roux en Y Gastric Bypass:
Its Advantages
It is reversible.
The rate of food absorption is lower.
Technically, it is easier than RNY Gastric Bypass surgery.
It creates a more permanent solution to Type 2 Diabetes and other co-morbid diseases.
The complication rate is low.
You are less likely to gain weight back.
Its Disadvantages
It should not be preferred in patients with reflux.
There is a possibility of bile reflux.
Gastritis and esophageal irritation (esophagitis) may occur due to reflux.
A lifelong intake of vitamins and iron may be required.
Assoc. Prof. Ahmet Tekin

General Surgeon
METABOLIC SURGERY